
- Information
- AI Chat
Psychiatric Nursing Care Plan
Med Surg 2 (Nurs 211L)
West Coast University




Preview text
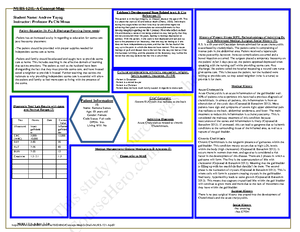
PSYCHIATRIC NURSING CARE PLAN TEMPLATE Student Astrid Hernandez Date 12/8/
Instructor Dinorah Rodriguez Course Mental Health Patient Initials A L Date of Admission 12/7/2020 Legal Status (Vol, 5150, 5250, Patient DOB 1/9/1997 Unit Psychiatric Conservatorship) 5150 Chronological and Apparent Age 25 Gender Female Ethnicity Hispanic
Allergies NKA
Height/Weight Temperature Heart Rate Respiration Rate Pulse Ox (O 2 Sat) Blood Pressure (location)
Pain Scale 1- (location, character, onset)
5’7/ 180 lbs 98 F (Oral) 88 bmp 17 98% 120/ 90 Left Arm
Pain is a 7 It is on the arm Patient describes pain as sharp Began yesterday.
Psychiatric Diagnosis and DSM 5 Diagnostic Criterion History of Present Psychiatric Illness:
The patient is diagnosed with Major Depressive Disorder Multiaxial Diagnostic System: Axis I : Major Depressive disorder Axis II : Acute Psychosis Axis III: N/A Axis IV : N/A Axis V : 30
Patient is a female, 25 years old currently working for a marketing company under the payroll department. The patient has been admitted to Larkin Psychiatric hospital by paramedics after having an acute mental breakdown followed by a suicide attempt. The patient was heard by neighbors throwing things and breaking things in her apartment while yelling and sobbing uncontrollably. When paramedics entered the patients apartment, she was found sitting on the railings in her balcony from her 34th floor apartment. She was attempting to jump and end her life. Patient has a history of counseling and
PSYCHIATRIC NURSING CARE PLAN TEMPLATE therapy. She was admitted to the hospital two years ago after ingesting a whole bottle of Tylenol in another suicidal attempt. Patient has an ongoing history of depression. The patient has stated feeling like there is no purpose in her life and feels there is no reason for her to be alive. Psychopathology of admitting and/or related psychiatric diagnosis Biophysical and/or related medical diagnosis
With APA citations
Erickson’s Developmental Stage With APA citations
In Major Depressive Disorder, mood thoughts and behavioral patterns are usually impaired for a long time. It usually impairs social functioning and quality of life. Major depressive disorder is usually identified by sadness, loss of interest of pleasures in daily life activity, changes in weight, sleep disturbances, physical impairment and alarming suicide rate. Major depressive disorder occurs when there is neurotransmitter deficiencies. This neurotransmitter deficiencies usually come from either serotonin or norepinephrine. Serotonin usually affects mood, sexual behavior, sleep cycles, hunger, and pain perception. While norepinephrine affects attention and behavior( Friedlander &Mahler, 2001).
The patient’s developmental stage based on the Erikson’s Psychosocial Stages is intimacy vs. isolation. In this stage, young adults need to form intimate, loving relationships with other people. Success is led by a strong relationship while failure results in loneliness and isolation(Orenstein & Lewis, 2020).
PSYCHIATRIC NURSING CARE PLAN TEMPLATE Patient is oriented to time, place, and where she is. The patient is able to recall recent events up until her admission to the facility. She knows my name and is able to spell it.
Patient is alert but very dull and uninterested. Patient stays in bed or most of the day and does minimal interaction with others. when patient does minimal interaction, responses are coherent and easy to understand. They are lacking necessary detail.
normal limits. Patient is able to name the days , weeks and months. Thee patient is able to spell simple words such as “world” and her very last name.
Thought Processes
Values and belief system
Hallucinations and Delusions Judgment and Insight
The patient does report slight experiences of depersonalization. The patient also shows illogical thinking in regard to life. Patient does believe she no longer has a purpose in her life.
The patient does not report any hallucinations or delusions.
The patient’s judgement and insight are not the best. The patient does seem to believe that the answers to her depression and stress is to end her own life. The patient doesn’t seem to think ther4e are other options. Mood and Affect: Mood or how they feel most days
Affect or how they felt at a given moment
Rapport
Facial and Emotional Expressions
Response to Failure on Test Items
Impulsivity
Anxiety
On most days, the patient reports feeling sad, melancholic, depressed and anxious. The patients affect seems to constantly be blunted. Patient seems to be indifferent. It goes along with sadness and depressive.
Patient’s rapport was initially difficult to establish but easier over time. Patient’s facial and emotional expressions range from sad to pessimistic. Patient will be said and tearful sometime, and at other times pessimistic with negative thoughts at other times.
Patient responds to test items unaffected. Impulsivity is very poor. The patient’s anxiety levels are moderate. Anxiety slightly elevate when asked about recent events regarding the suicidal attempt. The patient seemed anxious by sudden increase in speed of speech and slightly elevated voice.
Risk Assessment: Discharge Plans and Instruction: Teaching Assessment and Client / Family Education:
PSYCHIATRIC NURSING CARE PLAN TEMPLATE
Patient is a risk to self for the patient is suicidal. The patient already has two suicidal attempts on record and can potentially try again.
Patient will have a better understanding of disease process. Patient will go home to family who is her support system. Patients will have scheduled medication. Patient will continue counseling after discharge.
Patient will understand it is important to take medication. Patient will understand that counseling is also part of getting better. Patient will understand that although she is feeling better, she cannot stop the medication. She will also understand that it will take 4-6 weeks for her to feel full therapeutic effect of medication. Patient will also be able to distinguish stressors and triggers that send her into depressive moods.
Pertinent Lab Tests Results (normal ranges in parentheses)
Rationale for Abnormal
Valproic Acid (50 – 120 mcg/mL) N/A Lithium (0 – 1 mEq/L) N/A Carbamazepine (5 – 12 mcg/mL) N/A CBC (WBC with diff, ANC, RBC) within normal limits Urine Drug Screen Negative Thyroid Panel All within Liver Function (AST/ALT, LHD, Albumin, Bilirubin) within normal limits Kidney Function (BUN, creatinine) Within normal limits Blood Alcohol Level None in blood Diagnostic Test Results (with dates)
Rationale for Abnormals
N/A N/A
J
Substance Abuse and other Addictions Type: N/A Amount / Frequency: Duration: Last Used: Withdrawal Symptoms:
Type: Amount / Frequency: Duration: Last Used: Withdrawal Symptoms: C.A.G. Questionnaire
PSYCHIATRIC NURSING CARE PLAN TEMPLATE
Diagnosis . Planning Implementation Rationales for interventions Evaluation
1 for suicide related to psychiatric illness as evidenced by suicide attempt.
Nursing Diagnosis Definition: Patient is at risk for harming self due to major depressive disorder as seen with suicide attempt (Martin, 2019).
1 will refrain from attempting suicide.
2 will remain safe while in the hospital, with the aid of nursing intervention and support.
1 for patient to stay with family or friends. A hospitalization is considered if there is no one available. 2 and pills are removed by friends, relatives, or nurse.
3 patient to talk openly about feelings and help plan alternative ways of handling disappointment, anger, and frustration.
4 family and arrange for family crisis counseling.
Relieve isolation and provide safety and comfort.
provide safe environment , free from anything that can potentially harm them
gives the patient different ways to deal with strong feelings and emotions and get a sense of control of life.
4 ties. Lessens sense of isolation, gives contact from people who care for the patients. ( Martin, 2019).
1 feels sense of control over life and what actions she will take to handle future stressful situations.
2 feels less alone during family counseling with the support of her family.
- Ineffective coping related to impulsive use of extreme solutions as evidenced by destructive behavior towards self.
Nursing Diagnosis Definition: patient does not have appropriate coping techniques as
- Patient will report adequate supportive social contacts.
2 will name two effective ways to handle difficult situations in the
1 patient’s strengths and positive coping skills. 2. identify situations that triggers suicidal thoughts.
3 client’s social support
4 need for assertiveness training
- us e these to build an appropriate care plan.
2 targets for learning better adaptive coping skills. 3. have client try reaching out to at least two possible candidates. 4 people have a hard time getting needs met anger and frustration and anger can build up which can potentially lead to ineffective outlet of stress.
1 is building a support system.
2 showing positive coping skill through assertiveness training.
Diagnostic
Label
Contributing As evidenced by Factors
Related to Signs and
Symptoms
PSYCHIATRIC NURSING CARE PLAN TEMPLATE con be seen with suicide attempt (martin,2019).
future. (Martin, 2019).
PSYCHIATRIC NURSING CARE PLAN TEMPLATE
REFERENCES
Lewis, L., & Orenstein, G. (2020). Eriksons Stages of Psychosocial Development. Retrieved from
ncbi.nlm.nih/books/NBK556096/
Major depressive disorder: Psychopathology, medical management and dental implications. (2019). Retrieved from
sciencedirect/science/article/abs/pii/S
Martin, P. B. (2019, April 11). 3 Suicide Behaviors Nursing Care Plans. Retrieved from nurseslabs/suicide-behaviors-
nursing-care-plans/
PSYCHIATRIC NURSING CARE PLAN TEMPLATE
Psychiatric Nursing Care Plan
Course: Med Surg 2 (Nurs 211L)
University: West Coast University
This is a preview
Access to all documents
Get Unlimited Downloads
Improve your grades
