- Information
- AI Chat
SBAR-Fullsize-Nursing-Report-Sheet Post OP Assessment
Nursing (890)
Delta State University
Preview text
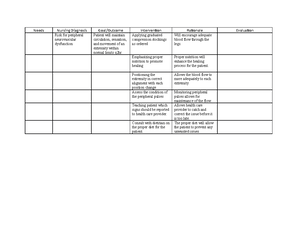
Post-Operative Assessment Form Name: ________________ DOB : _________Rm # _______ Age: ____ y/o M / F Surgical Procedure: ___________________________( Date: ______) Date Admitted: _____________ FULL CODE / DNR Today’s Date: _______________ Anesthesia: Gen / MAC / Spinal / Epid / Block Nurse Completing Form: ____________________________ Physician: _______________________ store.nursejanx/checkout/purchase-confirmation/ S Date: _____ Time: _______ V/S: ________________________________________________ Situation Time: _______ V/S: ________________________________________________ Time: _______ V/S: ________________________________________________ Time: _______ V/S: ________________________________________________ B PMH: DM / CHF / HTN / CAD / COPD / Asthma / Smoker / Drug Abuse Other: ____________________ Tests: MRI / X-Ray / CT / Echo EF: ____ Findings: ______________________________________ Background IV: Cath size #_____ IVF: NS / ½ NS / D5 ½ / D5 NS / LR / Abx Site: AC / FA / Hand / Wrist / UA IV Rate: _____ ml/hr Central: IJ / PICC / Port / Central Line Site: ________ Drips: Heparin / Blood / TPN Neuro Pain A & O x ___ / Confused / Restraints / Bed Alarm Level: MRSA Activity: Up ad lib / Assist x 1 or 2 / Bed-rest Location: C-Diff Walker / Cane Medication: ESBL PEARL Frequency: A Assessment Contact Isolation: Flu Droplet Neutropenic Universal Prec Extras: Respiratory O2 @ ___L NC / Room air / NRB / CPAP / BIPAP / Trach: _______ Breath Sounds: Clear / Diminished / Wheezing / Crackles / Coarse Treatments: Nebs / IS / CPT Cough: Productive / Non-productive Preop VS HR BP Temp RR O2 Cardiovascular VTE Prophylaxis Telemetry: __________ N/A SCDs / Foot Pumps Edema: None / Gen / Trace / 1+ / 2+ / 3+ / 4+ Heparin / Lovenox Pitting / Non-pitting Coumadin / Xarelto R / L / Bilateral Pulses: DP: Palpable / Non palpable Arms / Legs PT: Palpable / Non palpable Eliquis / None Ordered Daily Weight Strict I&Os Fall Risk Gastrointestinal Genitourinary Diet: Reg / Clear / Full / AHA / ADA / Soft / Renal / NPO Voiding / Foley / Incontinence / Anuria Hypo / Active / Hyper / Nausea / Vomiting / Diarrhea Clear / Cloudy Yellow / Amber / Bloody PEG tube ( pump / Gravity ) / Ostomy Last BM: ______ BRP / Urinal / Bedside Comm / Bedpan Dialysis: M Musculoskeletal Tu W Th F Sa Su Skin (Wounds & Dressings) Weakness: RUE / LUE / RLE / LLE Numbness: RUE / LUE / RLE / LLE Accucheck N/A AC B AC L AC D HS Labs AC&HS / Q6o / Q___o WBC Hct Hgb Drains Plt PT INR Chest Tube / JP / Hemovac / Penrose / Wound Vac Na K Cl Output: ______ mL Ca Serosanguinous / Sanguineous BUN Cr CO2 Glucose Albumin NG Tube Output: ________mL R Recommendation Scheduled Procedures: _____________________________________________________________________ Consults: SS / PT / OT / GI / Cards / Neuro / Nephro / Wound / Ortho / Psych / Pulm / Surg Discharge to: Home / Home Health / LTAC / Swing Bed / Rehab
SBAR-Fullsize-Nursing-Report-Sheet Post OP Assessment
Course: Nursing (890)
University: Delta State University