
- Information
- AI Chat
Health Assessment example paper
Patient Centered Care Practicum (NRSE 2351)
East Tennessee State University
Recommended for you




Students also viewed
Preview text
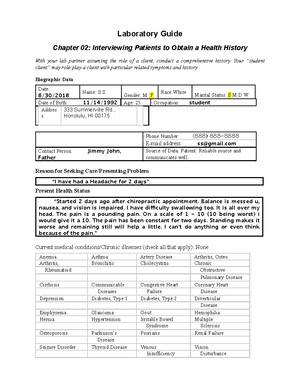
Running head: EXAMPLE 1 Health Assessment EXAMPLE Name East Tennessee State University EXAMPLE 2 Health History: Biographic Data Name: Gender: Address: Telephone numbers: (888) 888-8888, cell phone Birth date: Birthplace: Race/ethnicity: White (Caucasian) Religion: Marital Status: Single Occupation: Contact person: Source of interview data: patient, reliable Health History: Reason for Seeking Care: “I am having headaches that happen 2 times a week. I get nauseous and have sharp pain near my eyes.” History of Present Illness: Patient has experienced “headaches 2 times a week that makes me nauseous”. Patient states “there is pain near the front of my forehead and behind my eyes”. Patient describes pain as “sharp”, and “throbbing”. Patient rates pain “between a 7 and an 8”. Patient has limitations due to headaches, stating, “The headaches keep me from getting out of bed, and opening my eyes.” Patient states “headaches started 2 months ago”, and last “usually 4 to 5 hours, 2 times a week”. Patient is a teacher’s assistant and is “in the classroom, teaching, with the lights on, when I get my headaches”. EXAMPLE 4 Accidents/injuries: Reports none Immunizations: Childhood immunizations for school; Diphtheria date unknown; Pertussis date unknown; IPV date unknown; Hib date unknown; MCV date unknown; Pneumococcal date unknown; Influenza vaccine date unknown; Hepatitis A date unknown; HPV date unknown; Tetanus in 2008; Hepatitis B in 2008; MMR in 2003; Varicella in 2003 and 2009 Last examinations: Physical: June of 2018, reports “good results”; Vision: July of 2018, reports “vision is 20/20”; Dental: 1 year ago, reports “good results”; Last Menstrual Period: 08/20/18 to 08/24/18, reports “normal period”; Pap smear: none Obstetric history: Reports “never been pregnant” Family History: Mother: 55 years of age, alive and well, no chronic illnesses Father: 52 years of age, alive and well, no chronic illnesses MGM: deceased age 63 years, Non-Hodgkin’s Lymphoma cancer MGF: age unknown, alive and well, no chronic illnesses PGM: age 76, chronic problems; Diverticulitis, and Atrial Fibrillation PGF: deceased, age unknown, heart attack Maternal Aunts: none Maternal Uncles: 1, age 51, alive and well, no chronic illnesses Paternal Aunts: none Paternal Uncles: none Sisters: 1, age 19, alive and well Brothers: none EXAMPLE 5 Family and Social Relationships: Family and Social Relationships: o Lives with mother, father, and sister o No significant other o Patient considers family as “great” o Patient states “family is supportive of them” o Patient helps take care of their paternal grandmother, who is not in good health Diet/Nutrition: o Patient has 3 meals a day o Patient states appetite is “fine” o No diet o Patient “occasionally craves sweets” o Patient “does not drink a lot of water” Functional Ability: Patient can do the following with no problems: dressing, ambulating, toileting, shopping, bathing, cooking, eating, and housekeeping Mental Health: o Patient has stress from “starting nursing school” o Patient has stress from “grandmother being in the hospital” o Patient has mild anxiety o Patient “talks with friends to relieve stress” Personal Habits: denies drug use; denies smoking; consumes an alcoholic beverage “once a week”
Health Assessment example paper
Course: Patient Centered Care Practicum (NRSE 2351)
University: East Tennessee State University

