- Information
- AI Chat
Wirth NURS 355 Psych Exam 1 Study Guide
Psych-Mental Health Nursing (NURS 355)
Virginia Commonwealth University
Recommended for you




Related Studylists
Psych mental healthPreview text
Study hints: - Ask: “if I had to take care of this pt in real time, what would I have to do?” - Q’s starting w/ “why” are never correct answer (accusatory)
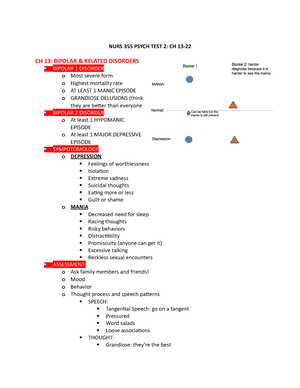
Chapter 1: Mental Health and Mental Illness ● Mental Health (positive) ○ Able to recognize own potential ○ Cope w/ normal stress ○ Work productively ○ Make contribution to community ● Traits of mental health: ○ Think rationally ○ Communicate appropriately ○ Learn ○ Grow emotionally ○ Be resilient ○ Have healthy self-esteem ○ Realistic goals & reasonable function w/in the individual’s role ● Resilience - “bounce back,” able to get back up & deal w/ difficulties ○ self-subjective – diff for everyone ○ Learned from facing trauma ■ In order to build - need to be taught & have tools to deal w/ stressors ○ Ability & capacity to secure resources needed to support well-being ○ Characterized by: ■ Optimism ■ Sense of mastery ■ Competence - knowledge & experience that helps you learn to deal w/ adversity ○ Essential to recovery ● Mental illness: ○ Disorders w/ definable dx ○ Significant dysfunction in mental functioning related to: ■ Development ■ Biological ■ Physiological disturbances ○ Culturally defined ○ Sad, mad etc. are normal emotions! Mental illness is defined as a decrease in the ability to perform daily tasks/functions
● Diathesis-Stress Model: ○ Diathesis = biological predisposition
○ Stress = environmental stress or trauma ○ Most accepted explanation for mental illness ○ Assertation: most psychiatric disorders result from a combination of genetic vulnerability & negative emotional stressors
● Primary prevention: build resilience - pt education ● Secondary prevention: active process - receiving treatment actively ● Tertiary prevention: maintain & manage pt’s baseline - (after we’ve stabilized) prevent mental health decompensation
● Incidence = # new cases at a given time ● Prevalence = # of cases regardless of when they begun ○ MDD = most common mental health disorder
● Lifetime risk = risk that one will develop a disease in the course of a lifetime ● Psychiatric mental health nurses (what the majority of mental health nursing is) ○ Promoting mental health through assessment, diagnosis, & treatment of behavioral & mental disorders
Chapter 2: Theories and Therapies ● Defense mechanisms and anxiety - (actually good) theory by Freud ○ Operate on unconscious level ○ Deny, falsify, or distort reality to make it less threatening ○ Only problematic if you ALWAYS use these ● Table 15: Defense Mechanisms (pg. 271)
Defense Mechanism Adaptive Use Maladaptive Use
Conversion is the unconscious transformation of anxiety into a physical symptom with no organic cause.
No example. Almost always a pathological defense.
A man becomes blind after seeing his wife enter a hotel room with another man.
Denial involves escaping unpleasant, anxiety-causing thoughts, feelings, wishes, or needs by ignoring their existence. Most used defense mechanism!
A man reacts to the death of a loved one by saying, “No, I don’t believe you,” to initially protect himself from the overwhelming news.
A woman whose husband died 3 years earlier still keeps his clothes in the closet and talks about him in the present tense.
Displacement is the transference of emotions associated with a particular person, object, or situation to another non threatening person, object, or situation.
A child yells at his teddy bear after being picked on by the school bully.
A child who is unable to acknowledge fear of his father becomes fearful of animals.
■ Positive reinforcement: giving a reward for a desired behavior ● Encouragement is enough & prob best - leaves room for intrinsic desire ■ Negative reinforcement: taking away something that’s bad as a reward → hoping will encourage good behavior ● should be followed by positive reinforcement (or won’t work) ○ Aversion therapy: punishment ■ E., time out, beating, phone away (removing a positive thing) ○ Modeling: exhibiting the behavior you want to see ○ Systematic desensitization: exposure therapy in a positive controlled environment, repeatedly & incremental ○ Flooding: direct exposure to your fear/stress stimulus all at once in real time ○ Biofeedback: biomonitors - HR, RR, BP - talk about stressors and & how to make level → teach pt how to maintain biological factors
● Cognitive theories: ○ Cognitive-behavioral therapy (CBT) ■ Therapist challenging pt’s narrative in order to change pt’s perception - offer suggestions to change perception ● Therapist helps pt align perceptions etc. to determine what the pt can do ■ The most widely used therapeutic modality of therapy ● Only if you don’t have a personality disorder
Humanistic theories ● Maslow’s Hierarchy of Needs:
● Biological model ○ Consider other influences that play a role in the development and treatment of mental disorders → Social, environmental, cultural, economic
● Brain stimulation therapies: ○ Electroconvulsive therapy (ECT) – electricity applied to the brain (like rebooting your computer) ■ Last resort tx for MDD, PTSD, schizophrenia ■ Before ECT prep: ● Pt heavily sedated ● Seizure precautions ● Code Cart ● Cardio monitoring - esp. RR & dysrhythmias(!!) ■ After ECT: ● #1 concern = physiologic function! ● Dysrhythmias ● Headache, confusion, N/V ● Temporary memory loss ○ Transcranial magnetic stimulation - repetitive (rTMS) (Jr. varsity version of ECT) ■ Tx for PTSD & depression ■ Less invasive than ECT → would try b4 trying ECT ● Outpatient procedure ■ Side Effects: Confusion, headache, temporary memory loss Developmental theories: ● Theory of psychosocial development (Erikson) - Personality continues to develop through old age ● Eight stages of development: ○ Trust vs. mistrust - 0.1 yrs ■ If needs dependably met, infants develop a sense of basic trust ○ Autonomy vs. shame and doubt - 1-3 yrs ■ “Me do it phase.” Toddlers learn to exercise their will & do things for themselves, or they doubt their abilities. ○ Initiative vs. guilt - 3-6 yrs ■ Preschoolers learn to initiate tasks & carry out plans, or they feel guilty about their efforts to be independent. ○ Industry vs. inferiority - 6-12 yrs ■ Children learn the pleasure of applying themselves to tasks, or they feel inferior. ○ Identity vs. role confusion 12-20 yrs ■ Teenagers work at refining their sense of self by testing roles & then integrating them to form a single identity, or they become confused about who they are. ■ Teenagers don’t have enough life experience to deal w/ stuff - resort to:
○ Definition: environment itself is therapeutic → helps the pt get better ○ Nurses - teamwork: ■ Routine supervision - managers/supervisors talk to nurses routinely ■ Consistency (nurses + pt’s) - hold pt’s to same standards ● “NCLEX standard” unit - Safety = # ○ Door & windows locked ○ Slant top doors & in-set water faucets ■ Can’t barricade ■ Can’t create ligature ○ Weighted/bolted furniture – not able to move ○ Individual rooms ○ 1:1 sitter for SI pt’s (w/ plan that’s executable on unit) ○ Q15 min rounds ○ Calm environment - NOT pt’s trying to fight
● Rights of hospitalized psychiatric patients ○ Every pt has the right to refuse – it’s just how long will they be allowed to refuse before the hospital takes legal action (tx is episode specific) - cuz pt can’t make informed decision about medical tx d/t mental illness ■ Insurance won’t pay for stay if pt isn’t being treated ○ Right to know what tx (med rights) ○ Patient’s need for safety must be balanced against patient’s rights as a citizen
● The rest of rights from the textbook: ○ Right to be treated with dignity ○ Right to be involved in treatment planning and decisions ○ Right to refuse treatment, including medications ○ Right to request to leave the hospital, even against medical advice ○ Right to be protected against harming oneself or others ○ Right to a timely evaluation in the event of involuntary hospitalization ○ Right to legal counsel ○ Right to vote ○ Right to communicate privately by telephone and in person
Chapter 5 - cultural implication:
Western tradition - USA ● Identity found in individuality ● Values: Autonomy, Independence, & Self-reliance ● Mind and body separate entities ● Disease has a cure, and treatment is aimed at the cause
● Time is linear ● Success is obtained in preparing for the future ○ When die: will & life insurance → don’t be a burden to everyone else when you die
Eastern tradition - Asian and Africa ● Family basis for identity ● Body-mind-spirit one entity ● Time is circular and recurring → Reincarnation ● Born into a fate; duty to comply ● Disease caused by fluctuations in opposing forces ○ Hot/cold, yin/yang Indigenous Culture - Native Americans ● Places significance on place of humans in natural world ● Basis of identity is the tribe ● Person is an entity only in relation to others ● Disease = lack of harmony between individual & environment
● Impact of culture on mental health - know these terms! ○ Enculturation: learning a culture - direct/indirect; pos/neg ○ Ethnocentrism: belief that your positioning/norms are the standard ○ Cultural imposition: imposing your culture on others w/ some type of force - physical or structural force ● People who are able to participate in their spiritual/traditions heal better/faster
Chapter 6 - legal and ethical considerations ● Bioethics = study of right/wrong (culturally determined) related to healthcare ○ Five Principles of Bioethics - if on exam, won’t be definition, will be examples of behavior ○ Beneficence: The duty to promote good ○ Autonomy: Respecting the rights of others to make their own decisions ○ Justice: Distribute resources or care equally ○ Fidelity (nonmaleficence): Maintaining loyalty and commitment; doing no wrong to a pt ○ Veracity: One’s duty to always communicate truthfully ○ Forgot to check on pt? Gotta go back and check on pt!
● Voluntary Commitment - sought by pt or guardian ○ Voluntary pt wants to leave & provider doesn’t agree? → independent assessor has to come & evaluate (RVHA, Henrico Co. Mental Health) ● Involuntary Commitment - w/o pt’s consent
■ HIV reporting - state dependent - some is if you have r/f exposure, some is only after exposure ○ Exceptions - when can confidentiality be broken? ■ Duty to warn & protect third parties → pt is a danger to self or someone else ■ Child & elder abuse reporting statutes ■ Workers compensation
● Negligence – Failure to do something - resulting in harm occurring to the pt, or near miss of harm to pt → 24 hrs to put in incident report (most places) ● Malpractice – Doing something you were never trained to do
● Assault = verbal ● Battery = physical - think bat for battery ● False imprisonment = impeding/blocking someones only exit ● Slander = verbal (can’t shit talk other hospital providers etc.) ● Libel = written
Guidelines for Ensuring Adherence to Standards of Care ● Duty to intervene & duty to report ○ Incompetence, impairment, or criminal activity ● If it isn’t documented - didn’t happen!! → don’t write generic nurses notes! ○ Accurate descriptions of pt’s behavioral status at the time it was written
Violence in the psychiatric setting ● Employers are not typically responsible for employee injuries from violent patients ○ In nursing, it is assumed that violence/injury comes w/ the job ■ Might get workers comp ○ Always document patient’s potential for violence ■ Pt hurt staff/another pt? Prob won’t be criminally charged - not guilty by reason of insanity ■ Communicate observations to colleagues
Chapter 7 - nursing process Standards of care: ● Standard 1: Assessment - how are mental health assessments different than normal med- surg assessments? ○ VV subjective ○ Cognitive impairment - may make assessment inaccurate ○ Age Considerations:
■ Assessment of Children - security, structure, support ■ Assessment of Adolescents - privacy, autonomy, insecurity ● Most behaviors are in effort to not be embarrassed ■ Assessment of Older Adults - warmer or quieter room ○ Gathering data: ■ Laboratory data - most in-pt psych units - pt’s screened for: ● health issues prohibiting them from being on psych unit ● health issues that are source of psych issues ■ MSE = Mental Status Exam ■ Spiritual/religious assessment - where we can ● Standard 2: Diagnosis - 3 components: ○ Problem (unmet need) ○ Etiology (probable cause) ○ Supporting data (S/S) ○ Lots of quoting the pt ● Standard 3: Outcomes Identification (didn’t go over) ● Standard 4: Planning - principles to consider when planning care ○ Safe - de-escalation first!! ○ Compatible & appropriate ○ Realistic & individualized ○ Evidence-based ● Standard 5: Implementation ○ Basic interventions: ■ Coordination of care ■ Health teaching & health promotion ■ Milieu therapy - environment itself is therapeutic to the pts ○ Advanced practice interventions: ■ Prescriptive authority & tx - psychiatrist, psych NP ■ Psychotherapy - LPC/LCS, NP, psychologists ■ Consultation ● Standard 6: Evaluation ○ Systematic ○ Ongoing ○ Criteria-based ○ How do we know pt getting better? Resolution of behavioral S/S
Chapter 8 - therapeutic relationships ● Fake it till you make it! → Confidence! Never panic in front of your pt ● “Trained to go” stance - one foot back → give space between you and pt ● No stethoscope, hoop earrings, lanyards, pens, necklaces
○ When nurse’s needs are met at expense of pt’s needs → tx of pt that’s convenient for nurse (w/o medical need for)
● Peplau’s model of nurse-pt relationship: ○ Orientation phase - warming up, getting to know, establishing boundaries ○ Working phase - reassuring, gathering additional evidence → trying to help pt see beyond this moment ■ E., Modeling behavior, med admin, interpersonal communication, therapy ○ Termination phase - ready for discharge ■ Safety, coping strategies = 2 best indicators of readiness to leave ■ Can pt facilitate to you what they’ll do if they get to this point again?
● Factors that help nurse-pt relationship: ○ Consistency ○ Pacing ○ Listening ○ Initial impression → Can be influenced by our biases ■ Need context b4 you can dx ● Factors that promote pt growth: ○ Empathy: - putting yourself in their shoes - knock knock “hey, I didn’t tell you I was coming, but I came to check on you” ○ (not) Sympathy: “awww, I'm so sorry”
Chapter 9 - therapeutic communication ● Therapeutic communication Q answer structure: ○ 1) Acknowledge pt’s issue/grievance ○ 2) Ask open-ended Q’s that allows pt to tell more ● E., “I can see that you seem frustrated, can you tell me more about how you feel?” ● 1 exception: Pt exhibits overt or covert statements of self-harm or harm to others ○ Best response = “are you having thoughts of harming yourself/others?” → then use therapeutic structure
Chapter 11 - childhood and neurodevelopmental disorder ● Etiology ○ Psychological factors: ■ Temperament - your personality (can see at v young age) - how you respond to stressors ■ Resilience ○ Environmental factors - can contribute to increased r/f developing these
disorders ■ Witnessing violence ■ Neglect and abuse ■ Bullying ● General interventions for children and adolescents ○ Behavioral interventions - modeling/changing behavior ○ Play therapy - can reveal things they’ve seen ○ Bibliotherapy - books written for kids that explain medical issues in way they can understand ○ Journaling - for adolescents ○ Music therapy - really helpful! ○ Family interventions - family therapy ○ Psychopharmacology ○ Disruptive behavior management ● Advanced practice interventions ○ Group therapy ■ Younger children: uses play and ideas ■ Older children: combines play, learning skills, and talk ■ Adolescents - processing-type therapy ● CBT = best; if adolescents will listen to you!
● Autism spectrum disorder (ASD) - stereotypical (for testing purpose) ○ Deficits in social relatedness & relationships ■ Moderate-severe ASD: pt doesn’t respond to anyone ■ Stereotypical repetitive speech ■ Obsessive focus on specific objects - Hyperfocus on 1 thing indefinitely ■ Over adherence to routines or rituals - not going to go well ■ Extreme resistance to change ■ Hyper- or hypo-reactivity to sensory input ■ Appears in early childhood (miss developmental milestones) ○ Implementation - Neg reinforcement, aversion therapy ○ Evaluation - how do we know tx is effective? Pt is able to resist their maladaptive behaviors ■ E., okay w/ diff outfit/meal/etc.
● ADHD - stereotypical for testing purpose ○ Typically - don’t do well in school ○ Classic S/S: Inattention, Impulsivity, Hyperactivity, Short attention span ○ Assessment: (ADHD behavior in 2+ locations for dx) ■ Level of physical activity ■ Attention span
Wirth NURS 355 Psych Exam 1 Study Guide
Course: Psych-Mental Health Nursing (NURS 355)
University: Virginia Commonwealth University



- Discover more from: