
- Information
- AI Chat
Introduction TO Medical Protozoology
Principles of Public Health (APP 709)
Adekunle Ajasin University
Students also viewed
- LIST OF Cases IN Profesional Ethics AND Skills AND THE RPC
- IT Work Experience at Lagos State Ministry of Works and Infrastructure - Electrical Services Department
- Aaua Siwes report compiled by Olatunji O
- Effective-interviewing-rvs
- Mistake Cases Contract Law Law Teacher
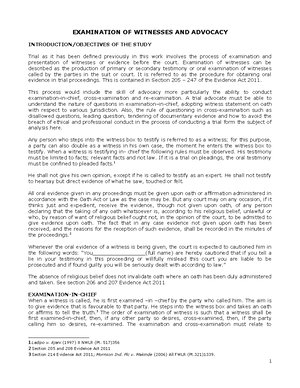
- Notes on Examination OF Witnesses AND Advocacy
Preview text
INTRODUCTION TO MEDICAL
PROTOZOOLOGY
What Are Protozoa?
Protozoa are unicellular eukaryotic micro-organisms. Protozoa possess typical eukaryotic organelles and in general exhibit the typical features of other eukaryotic cells.
Protozoans exhibit a wide variety of morphologies. Shapes range from the amorphous and ever-changing forms of amoeba to relatively rigid forms dictated in part by highly ordered cytoskeletons or secreted walls or shells. Several protozoan species express photosynthetic or other pigments and thus are coloured. Many protozoan species exhibit complex life cycles with multiple stages. Sometimes the different life cycle stages are so dissimilar that they have been mistaken for completely different species. The vast majority of protozoa are microscopic. However, they do exhibit an incredibly large range of sizes. Protozoa are found in moist environments virtually everywhere. As a group, the protozoa are extremely adaptable. Individual species, though, generally have specific niches. Like all other organisms, protozoa must be able to acquire and metabolize nutrients from their environment (i., heterotrophic). Many protozoa simply absorb solutes (i., osmotrophy) from their media, while some are scavengers that ingest solid material (i., phagotrophy). Predatory protozoa either actively hunt down or passively ambush other organisms (typically bacteria or other protozoa). Some protozoa are photosynthetic and can capture the energy of the sun and convert it to
usable chemical energy (i., autotrophic or phototrophic). Many protozoa are not restricted to a single feeding mechanism and can utilize combinations of the above (i., mixotrophic).
Protozoa can also be viewed as free-living or symbiotic.
Motility and the Cytoskeleton
Cilia and flagella are subcellular structures which propel protozoa through a fluid medium. Flagella are long whip-like structures which propel the organism as a result of wave-like beat which is propagated through their length. Flagellated protozoa typically have one or a few flagella per organism. In contrast, ciliated protozoa are usually covered with rows of numerous cilia. The beats of these cilia are coordinated and function like oars to propel the organism. Cilia and flagella can also assist in the procurement of food, reproduction and other functions. In contrast to the swimming exhibited by flagellates and ciliates, amoeba are protozoa that crawl along a solid substratum in a fashion known as 'ameboid movement'. The amoeba projects out a pseudopodium, or false foot, from the cell body. The pseudopodium attaches to the substratum and then pulls the rest of the cell body forward. Apicomplexa also crawl along a substratum, but by a different mechanism than the amoeba. The mechanism of this so-called 'gliding motility' is just beginning to be understood and probably involves both microfilament and microtubule based cytoskeletal systems. Apicomplexa also exhibit intracellular forms and invasion of the host cell also involves this gliding motility.
Cellular motility involves force generation through either the microtubule- based cytoskeletal elements or the microfilament-based cytoskeletal elements. This is true for protozoa and other eukaryotes. The involvement of microtubules and microfilaments in both cell shape and cell movement make these subcellular structures more analogous to the musculoskeletal system.
Reproduction
Modes of Motility
Mechanism Subgroup ameboid movement amoebas flagella flagellates cilia ciliates gliding motility sporozoa
Modes of Reproduction
Asexual Binary Fission Multiple Fissions Budding Sexual Fusion of Gametes Conjugation
The kinetoplastids are a widespread group of flagellated protozoa. Members of this group parasitize virtually all animal groups as well as plants and insects. There are also free-living kinetoplastids which feed on bacteria in aquatic, marine and terrestial environments. The kinetoplastids are likely a monophyletic group which are related to the euglenids. Three distinct kinetoplastids cause human disease: African typanosomes (African sleeping sickness), Trypanosoma cruzi (Chagas' disease), and Leishmania species (leishmaniasis). All three are parasites of the blood and/or tissues of the human host and are transmitted by arthropod vectors.
The major distinguishing feature of this group is a subcellular structure known as the kinetoplast. The kinetoplast is a dark Giemsa-staining structure which is distinct from the nucleus. The size of the kinetoplast will vary according to species. The kinetoplast is found near the basal body which is located at the base of the flagellum. Because of this location near the flagellum, it was previously believed that the kinetoplast was somehow associated with cell movement--hence the name. However, the kinetoplast is actually a distinct region of the mitochondria and is not involved in motility. The staining of the kinetoplastid is due to mitochondrial DNA. Typically, the kinetoplastids are depicted as long slender organisms. However, the kinetoplastids exhibit several morphological forms which are defined by the position of the kinetoplast in relation to the nucleus and the length of the undulating membrane. Cellular features of the kinetoplastids include:
A single flagellum present in many of the morphological forms. A paraxial rods runs along beside the axoneme. The flagellum is sometimes attached to cell body to form undulating membrane. The flagellum emerges from a flagellar pocket. Endo- and exocytosis is limited to this flagellar pocket. A single and often branched mitochondria with discoid (rarely flattened or tubular) cristae characterized by the ktDNA. The presence of a peroxisome-like organelle called the glycosome in which glycolysis occurs.
Kinetoplastids Causing Human
Disease
African trypanosomes
(African sleeping sickness)
Trypanosoma cruzi
(Chagas' disease)
Leishmania species
(leishmaniasis)
A cytoskeleton composed of subpellicular (also called cortical) microtubules which run the length of the organism.
Morphological Forms
Several different morphological forms of kinetoplastids are observed. These various morphological forms are associated with different life cycle stages in the various species. The different forms are distinguished by the position of the kinetoplastid in relation to the nucleus and the presence or absence of an undulating membrane. The four major morphological forms found in kinetoplastids which cause human disease are:
trypomastigote
The kinetoplast (kt) is located on the
flagellum pulls the organism.
amastigote
The parasite is more spherical in shape and has no free flagellum. A basal body (bb) and the base of the flagellum is still present. The kinetoplast (kt) is usually detectable as a darkly staining body near the nucleus (Nu). This form is a non-motile intracellular stage.
AFRICAN TRYPANOSOMIASIS
African trypanosomiasis, also known as African sleeping sickness, exhibits a patchy distribution in equatorial Africa depending upon specific topographical features and the presence of the vector. The control of African trypanosomiasis is complicated by poverty, political instability, and civil wars often found in areas endemic for the parasite and vector. An estimated 60 million people in 36 nations are at risk of infection. The incidence of the disease had been increasing from the mid-1960s to the end of the 20th century with an estimated 300,000-500,000 cases occurring annually in 1998. However, increased awareness and programs initiated by the WHO have led to a decreasing incidence and in 2009 there were less than 10,000 cases (Simarro et al, 2011).
The parasites responsible for causing African sleeping sickness belong to a group of closely related trypanosomes in the Trypanosoma brucei species complex. Three morphologically indistinguishable species are recognized:
T. brucei infects game animals/livestock (causes nagana) T. rhodesiense causes E. African trypanosomiasis T. gambiense causes W. and Central African sleeping sickness
(Some authors consider these as subspecies: T. brucei brucei, T. b. rhodesiense, T. b. gambiense.)
T. brucei is a natural parasite of wild game in Africa and are non-infective to humans. This inability to infect humans is due to a 'trypanosome lytic factor' found in human sera (tulane/~wiser/protozoology/notes/TLF). T. brucei and two morphologically distinct trypanosmes, T. vivax and T.
congolense, are major pathogens for wild and domestic animals and have far reaching effects on raising livestock. In fact, although trypanosomiasis can be a devastating human disease, the greatest impact of trypanosomiasis on human health is at the agricultural level. Large areas of Africa are unsuitable for raising cattle and other livestock due to the presence of the tsetse vector and the transmission of trypanosomes. This contributes to protein deficient diets among the indigenous population.
As the names imply, T. gambiense and T. rhodesiense are distinguished by their geographical distributions. T. rhodesiense is found in East Africa and T. gambiense is found in West and Central Africa. (Rhodesia is the former name for Zimbabwe.) The restricted distributions of the African trypanosomes are determined by the vectors. African trypanosomes are transmitted by several species within the genus Glossina, commonly known as the tsetse. In addition to being transmitted by different vectors, T. gambiense and T. rhodesiense are distinguished by animal reservoirs, epidemiology, and disease virulence (Table).
Major Differences Between African Trypanosome Species
Attribute T. rhodesiense T. gambiense tsetse vector G. morsitans group G. palpalis group ecology dry bush, woodland rainforest, riverine, lakes transmission cycle ungulate-fly-human human-fly-human non-human reservoir wild animals domestic animals epidemiology sporadic, safaris endemic, some epidemics disease progression rapid, often fatal slow (~1 yr) acute ⇒ chronic parasitemia high low asymptomatic carriers rare common
The tsetse vector of T. rhodesiense is found in woodland or dry bush environments. Its natural vertebrate host is the antelope and other wild ungulates. Disease transmission depends upon coming in contact with infected vectors and is often associated with hunters or safaris. T. rhodesiense is primarily a zoonosis and little human-fly-human transmission occurs. The disease typically progresses rapidly and is often fatal without treatment. Although variants of T. rhodesiense which cause a slowly progressing chronic disease have been identified (MacLean et al, 2004, Infect. Imm. 72,7040). Molecular data suggest that T. rhodesiense may be a host-range variant of T. brucei.
T. gambiense is transmitted by vectors found along rivers and lakes which are often in close proximity to human habitation. Consequently, the disease tends to be endemic and domestic animals may serve as reservoirs. The disease is much less virulent and is characterized by a slow progression from an acute disease to a chronic disease. It is believed that T. gambiense has been associated with humans for much longer than
The focus in medical parasitology courses tends to be on the complex interactions between the parasite and the human host which result in pathology. However, parasites also interact with and undergo complex developmental processes in the vector. Vectors are more than 'flying syringes'. (Although T. evansi, a trypanosome infecting horses and camels, is transmitted mechanically by horseflies.) One problem for the trypanosome is that it must move from the gut to the salivary glands of the tsetse. The exact mechanism by which the parasite migrates from the tsetse gut to the saliva glands is not known. Two routes have been proposed: 1) the classical route in which the parasite 'backtracks' through the digestive system and migrates up the salivary duct, or 2) the direct route in which the parasite penetrates the peritrophic membrane and gut epithelium to gain access to the hemolymph.
After reaching the salivary glands the procyclic trypomastigotes transform into epimastigotes (E) and attach to epithelial cells via their flagella. The epimastigotes probably undergo further replication within the salivary gland. The epimastigotes are non-infective for the mammalian host and they must first mature into metacyclic trypomastigotes (MT). During this maturation the surface coat is reformed, the mitochondria lose their cristae and the parasite detaches. These trypomastigotes are free within the lumen of the salivary gland waiting to be transferred to a vertebrate host when the tsetse feeds again, thus completing the life cycle.
Antigenic Variation
The observation that an extracellular parasite which is found in the bloodstream causes a long-lasting chronic disease poses a paradox. Normally the host immune system is quite efficient at generating antibodies against infectious organisms and eliminating them from the circulation. In this regard, a characteristic of African trypanosomiasis is a fluctuating parasitemia (Figure, upper left). In other words the number of parasites in the circulation dramatically rises and falls. Generally, fever and other clinical symptoms are associated with the peaks in parasitemia. Further examination of parasites obtained from successive peaks reveals that they are antigenically distinct, or exhibit variant antigenic types (VAT).
The VAT are determined by a protein known as the variant surface glycoprotein (VSG). VSG is an abundunt protein (10 7 copies per cell) and is a major component of the 12-15 nm thick electron dense 'surface coat' covering bloodstream trypomasigotes. The parasite is estimated to have more than 1000 distinct VSG genes (occupying ~10% of the trypanosome's genome). Periodically the parasite will express a different VSG gene which is antigenically distinct from the previously expressed VSG with a switch rate of approximately 10-2 per cell per generation. Comparing the sequences of the various VSG genes reveals a N-terminal variable domain and a C-terminal conserved domain (Figure, lower left). Also at the C-terminus is a GPI anchor which is imbedded into the lipid bilayer of the plasma membrane. The VSG molecules fold and pack together in a manner so that the conserved C-terminal region is not directly accessible and that only the varible N-terminal region is exposed to the host immune system (Figure, right).
VSG is immunogenic and antibodies against VSG do lead to parasite elimination. Switching expression to another VSG results in a new surface coat which is now not recognized by the host antibodies. These parasites will then rapidly increase in number until the host mounts an immune response against the new VSG. The large repertoire of antigenically distinct VSG proteins means that the parasite stays one step ahead of the host and avoids complete elimination by the immune system.
Three distinct pools of VSG genes are found in the genome of the African trypanosome (Figure). The majority of the VSG genes are found in long tandem arrays of repeated genes in subtelomeric locations on the chromosomes. Approximately 200 copies of VSG genes are found at the telomeres of the mini-chromosomes. African trypanosomes contain approximately 100 mini-chromosomes of 50-100 kilobases which only code for VSG. Another 30-40 VSG genes are found in expression sites. There are two types of expression sites corresponding to the two life cycle
(see life cycle). The expression of VSG and the surface coat is a preadaptation of the parasite for the vertebrate host.
Another mechanism of VSG switching involves telomere exchange between the telomere with the active expression site and a telomere of a silent expression site or the telomere of a minichromosome. The exchange of the telomeres results in the expression of a previously silent gene and the silencing of the previously expressed gene.
The third mechanism of VSG switching involves a duplicative transposition of these VSG genes into the active expression site. The archive copy of the VSG gene is copied and the template remains intact. The copied gene then replaces the gene in the active expression site by a gene conversion process.
Sequencing of the genome of African trypanosomes revealed that relatively few (approximately 7%) of the VSG genes are intact functional genes, whereas the majority of the VSG genes have frame shift errors or in-frame stop codons. These pseudogenes undergo an intragenic recombination which can restore the coding sequence. The formation of these chimeric genes also leads to the formation of novel VSG molecules. This gives the African trypanosome an enormous potential to generate diversity. Thus the repertoire of VSG genes is continuously changing in that new variants are continuously being created whereas recently expressed variants are being lost due to duplicative transposition (i., gene conversion).
See also:
D. Horn and R. McCulloch (2010) Molecular mechanisms underlying the control of antigenic variation in African trypanosomes. Curr Opin Microbiol 13(6): 700–705. J. Taylor and G. Rudenko (2006) Switching trypanosome coats: what's in the wardrobe? Tr. Genetics 22, 614-620.
Disease Course and Symptoms
Infection with African trypanosomes can result in disease manifestations ranging from asymptomatic or mild to a severe fulminating disease. T. rhodesiense is more likely to cause a rapidly progressing and fulminating disease than T. gambiense. T. gambiense tends to cause a slow progressing disease which may either be self-limiting or develop into a chronic disease involving the lymphatics and the central nervous system (CNS). The infection is almost always fatal with few documented cases of individuals clearing the parasites and surviving.
The infection is initiated when metacyclic trypomastigotes are introduced from the saliva of the tsetse into the bite wound. Generally there is an asymptomatic incubation period of 1-2 weeks in which the trypomastigotes are replicating within the tissue near the site of the bite. Occasionally, a local inflammatory nodule known as a 'trypanosomal chancre' is observed during this period. Chancres are usually tender and painful and ulceration may occur.
The trypomasigotes will invade the capillaries and enter the circulatory system during this incubation period and continue to replicate within the blood of the human host. The establishment of this acute blood stage infection is characterized by irregular episodes of fever and headache. In the case of T. gambiense the number of parasites in the blood tends to be very low and often the infected person exhibits no symptoms, whereas most persons infected with T. rhodesiense will exhibit much higher parasitemias and a more pronounced fever sometimes associated with rigor.
Disease progression is often characterized by invasion of the lymphatics in T. gambiense infections. Symptoms during the lymphatic stage include enlarged lymph nodes (particularly post-cervical group), weight loss, weakness, rash, itching, and edema as well as the continued intermittent febrile attacks. Higher parasitemias are often associated with the symptomatic periods. The infection can spontaneously resolve during either the blood stage or the lymphatic stage. There is usually little evidence of lymphatic involvement in T. rhodesiense infections. In general, the symptoms during the earlier stages of the infection tend to be non-specific (fever, malaise, headache, weakness) and may infect multiple organs.
A hallmark feature of African trypanosomiasis is the invasion of the CNS and nervous system impairment. Trypanosomes crossing the blood-brain barrier result in a generalized meningoencephalitis characterized by progressively worsening symptoms. Indications of nervous impairment include: apathy, fatigue, confusion, somnolence, and motor changes (such as tics, slurred speech, and incoordination). The changes in sleep patterns are often characterized by extreme fatigue during the day and extreme agitation at night. Generally it is 6-12 months (or even years) after the infection before the neurological symptoms start to become apparent in the case of T. gambiense. Neurological manifestations can occur within weeks after T. rhodesiense infections. If untreated, the CNS stage of the disease will almost always progress to include convulsions or
Disease Progression
1-3 week incubation period (± trypanosomal chancre) acute blood stage infection characterized by intermittent fever and headache invasion of lymphatics characterized by wasting and other symptoms CNS involvement and nervous impairment convulsions or coma leading to death
infections. The trypanosomes are more likely to be detected during symptomatic periods (eg., during febrile episodes). In the absence of detectable parasites, travel or residence in an endemic area combined with the symptoms discussed above can be used as a presumptive diagnosis.
Because of the low parasitemias exhibited during T. gambiense infections it is often not possible to detect parasites by standard thin and thick blood smears. Techniques to increase the sensitivity of detection are often needed (Box). For example, looking at fresh whole blood mounts may increase the sensitivity due to the distinctive movement of the trypomastigote. Another method to increase sensitivity is to centrifuge the blood in a microhematocrit tube. The parasites are enriched in the 'buffy coat' which is the band of white cells directly about the packed erythrocytes. The tube is then broken at the buffy coat and Giemsa- stained blood smears are prepared from these cells. Inoculation of mice or rats with patient blood and looking for the development of parasitemia is also possible. This generally works much better for T. rhodesiense infections than T. gambiense infections.
The miniature anion-exchange centrifugation technique (mAECT) is another method used in the diagnosis of human sleeping sickness. Blood is passed through an anion exchange column. Blood cells are more negatively charged than the trypanosomes and they are retained on the column. The trypanosomes pass through the column and are collected at the bottom of a sealed glass tube by low-speed centrifugation. The tip of the glass tube is then examined in a special holder under the microscope for the presence of trypanosomes. The large blood volume (300 μl) enables the detection of less than 100 trypanosomes/ml. Although highly sensitive, the manipulations are somewhat tedious and time-consuming.
One important issue in diagnosis of African trypanosomiasis is to distinguish the late encephalitic stage of the disease from the early stage. This is important since the treatment is different depending on whether
Parasite Detection in Blood
Giemsa stained thin or thick smears fresh (characteristic movement) buffy coat (microhematocrit) inoculate rats or mice mini-anion exchange centrifugation technique (mAECT)
there is CNS involvement (see below). Criteria for CNS involvement include detection of parasites in the cerebral spinal fluid (CSF) or elevated white blood cells (>5/microliter) in the CSF. There is some controversy in regards to the exact level of white blood cells in the CSF should constitute a classification of CNS involvement.
Treatment
Suramin and pentamidine are the recommend drugs during the acute stage without CNS involvement, whereas melarsoprol or eflornithine are recommend if the CNS is involved (Table). Pentamidine is less toxic than suramin. However, it is not effective against T. rhodesiense. All four of these drugs are provided free of charge by the World Health Organization through public and private partnerships with pharmaceutical firms. The prognosis is generally excellent if treatment starts during the acute stage.
Drug Use Drawbacks
Pentamidine Effective against early-stage gambiense disease Adverse side effects Non-oral route
Suramin Effective against early-stage gambiense and rhodesiense disease
Adverse side effects Non-oral route
Melarsoprol First line drug for late-stage gambiense and rhodesiense disease involving CNS
Adverse side effects, especially encephalopathy Fatal in 1-5% of cases Parasite resistance Non-oral route
Eflornithine Effective against late-stage gambiense disease involving CNS High cost Not effective against T. rhodesiense Non-oral route - has to be given intravenously (needs hospitalization for 14 days)
The drugs used to treat trypanosomiasis are less than ideal due to problems with toxicity and other drawbacks (Table). For example, melarsoprol, an arsenical based drug, has been used for more than 50 years despite it relatively high toxicity (up to 5% of patients die from the drug treatment). Furthermore, the treatment course is long (minimum 10
are impregnated with biodegradable insecticides in order to kill any flies that land on them. The strategy is to place the traps or targets around a village or other areas such as along riverbanks where bathing and washing activities take place or along paths. This will lead to a reduction in the number of tsetse in that vicinity. Traps and targets are also advantageous in that there is less environmental impact than widespread insecticide spraying or clearing brush from large areas. Although this strategy is relatively low-tech, it does require community awareness and participation. The traps and targets need to be maintained and replenished with attractants and insecticides.
Reviews on African Trypanosomiasis:
Kennedy, PGE (2013) Clinical features, diagnosis, and treatment of human African trypanosomiasis (sleeping sickness). Lancet Neurol 12, 186-94. Malvy, D and Chappuis F (2011) Sleeping sickness. Clin Microbiol Infect 17, 986-95.
LEISHMANIASIS
Several species of Leishmania are capable of infecting humans and causing disease. Leishmaniasis is expressed as a myriad of disease manifestations which depend upon parasite species, host responses, and poorly understood host-parasite-vector interactions. The different species and various clinical outcomes are also dependent on the geographic area and ecological setting. The number of reported cases and geographical areas in which leishmaniasis is endemic have been increasing.
Leishmania Incidence
350 million at risk 12 million infected 1-2 million clinical cases
Life Cycle
Like other kinetoplastids, Leishmania are transmitted by a hematophagous arthropod known as a sand fly. Two different genera of sandflies transmit Leishmania: Phlebotomus (Old World) and Lutzomyia (New World). Sandflies are 'pool feeders' and promastigotes are transferred to the vertrebrate host during feeding. The promastigotes are not in the salivary glands, but found in the anterior portion of the gut and pharnyx. Infection of the sandfly leads to a breakdown in a valve at the
entrance to the midgut. When the sandfly takes a blood meal the valve cannot close and blood moves back into the mouthparts and the bite wound. This regurgitation like activity results in an expulsion of promasitigotes from the anterior portions of the sandfly gut into the bite wound of the mammalian host.
Within the vertebrate host the promastigotes are phagocytosed by macrophages or other 'professional phagocytes'. The parasite cannot actively invade host cells and is dependent upon the phagocytic activity of the host cell. Therefore, Leishmania is predominantly found in macrophage-like cells. This parasite-containing phagosome, as do other phagosomes, fuses with a lysosome. Normally a pathogen is destroyed in the resulting phagolysosome, but Leishmania is resistant to the acidic pH and hydrolytic enzymes present in the phagolysosome. In addition, the parasite shuts down the generation of reactive oxygen intermediates by the macrophage.
The promastigote converts to an amastigote within the phagolysosome by losing its flagellum and becoming more spherical. These amastigotes replicate by binary fission and fill up the infected macrophage. Amastigotes are release from the host cell and taken up by another macrophage leading to another round of replication. The release of the
Introduction TO Medical Protozoology
Course: Principles of Public Health (APP 709)
University: Adekunle Ajasin University






- Discover more from:



Students also viewed
- LIST OF Cases IN Profesional Ethics AND Skills AND THE RPC
- IT Work Experience at Lagos State Ministry of Works and Infrastructure - Electrical Services Department
- Aaua Siwes report compiled by Olatunji O
- Effective-interviewing-rvs
- Mistake Cases Contract Law Law Teacher
- Notes on Examination OF Witnesses AND Advocacy