- Information
- AI Chat
Sabrina Vasquez v Sim Complete Care Plan
Nursing Care of the Childbearing Family (NURS 125)
Raritan Valley Community College



Preview text
DESCRIBE DISEASE PROCESS AFFECTING PATIENT (INCLUDE PATHOPHYSIOLOGY OF DISEASE PROCESS)
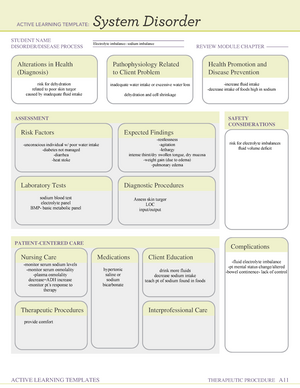
Pneumonia: Infection of the pulmonary tissue including the interstitial spaces, aviola an bronchioles. It is common in childhood but
occurs more frequently in early childhood. Clinically pneumonia may occur either as a primary disease or as a complication of
another illness. The causative agent is either inhaled into the lungs directly or comes from the bloodstream wong's essentials of
pediatric nursing 1
Asthma: A respiratory condition marked by spasms in the bronchi of the lungs, causing difficulty in breathing period it usually results
from an allergic reaction or other forms of hypersensitivity. Characterized by chronic inflammation, bronchoconstriction, an
bronchial hyperresponsiveness. Most common respiratory disorder in childhood
DIAGNOSTIC TESTS (REASON FOR
TEST AND RESULTS)
PATIENT INFORMATION ANTICIPATED PHYSICAL FINDINGS
Chest X-Ray: Allows HCP to
diagnosis pneumonia and assess the
location and extent of infection
SV results showed RLL
pneumonia w effusion
Pulse Oximetry : Monitor O
saturation levels
SV at 94% with 2L/min O2 vi
nasal cannula
Sputum Culture: SHOULD be
ordered to better determine type of
infection.
CBC w/ dif : SHOULD be ordered to
determine if there is a left (bacterial)
or right shift (viral) and levels of
neutrophils, changes in lymphocytes
monocytes increase is viral.
Neutrophils and bans are bacterial.
Increase Esinophils are expected
fining with asthma.
Sabrina Vasquez; 5 years old. Hispanic
CC : 39 C (102) temperature.
Dx: Pneumonia, asthma
Hx: asthma (moderate intermittent)
Mother reports; SV had an upper respiratoruy
infection for the past few days,exacerbating
her asthma and causing several athma attacks
requiring use of inhaler at home. This moring
her mother reports her temperature rose to
102, therefore she brought her into the ED.
She was placed on oxygen via nasal cannula at
2 L/min.
Received a 380-mL bolus of normal saline and
an
Administered albuterol nebulizer treatment at
1700.
o This improved her oxygen saturation
to 94%.
The chest x-ray revealed right lower lobe
pneumonia with effusion.
An intravenous infusion of KLC in D5NS is
infusing at 61 mL/hr.
Sabina just got settled in bed, and her mother
is at the bedside.
High fever
Cough can be
unproductive or
productive of white
sputum
Tachypenea
Intercostal retractions and
nasal flaring
Chest pain
Dullness upon percussion
Adventitious breath
sounds expiratory
wheezes (rhonchi, fine
crackles)
Pale color that progresses
to cyanosis
irritability, restless,
lethargic
abdominal pain, diarrhea,
lack of appetite and
vomiting
ANTICIPATED NURSING INTERVENTIONS
Monitor airway, breathing, circulation (ABCs)
o Reassess respiratory status when changes in status are noted
o Allow patient to assume a position of comfort
o Elevated HOB if possible
Administer oxygen to maintain saturations as ordered
Administer medications as ordered
Monitor response to rescue and prn medications
Swallow evaluation if cause is aspiration
Venous thromboembolism (VTE) prophylaxis, if hospitalized
Nothing by mouth in cases of respiratory failure or of aspiration from impaired swallowing ability
High-calorie, high-protein
Soft, easy-to-chew foods
Adequate fluids
1 "Wong's Essentials of Pediatric Nursing - 10th Edition." Ch. 21, p 653, para 8, elsevier/books/wongs-essentials-of-
pediatric-nursing/hockenberry/978-0-323-35316-8.
"RN Nursing Care of Children Study Package." store.atitesting/product.aspx?zpid=1631.
PATIENT EDUCATION WORKSHEET
NAME OF MEDICATION, CLASSIFICATION, AND INCLUDE PROTOTYPE
MEDICATION: Albuterol sulfate
CLASSIFICATION: Brochodilator / Adrenergics
PROTOTYPE: Albuterol (Trade: ProAir HFA, Proventil, HFA, Ventolin HFA)
SAFE DOSE OR DOSE RANGE, SAFE ROUTE
Patient Dose: Albuterol 2 milligrams in 2mL of NS ; safe dosage is 2 t.i or q.i, therefore this is a safe dosage PO (Children 2–6 yr): 0 mg/kg 3 times daily (not to exceed 2 mg 3 times daily initially); may be carefully ↑ to 0 mg/kg 3 times daily (not to exceed 4 mg 3 times daily). Solution for inhalation Children ages 2 to 12 weighing more than 15 kg: 2 mg by nebulizer given over 5 to 15 minutes t.i. or q.i., with subsequent doses adjusted to response. Don’t exceed 2 mg t.i. or q.i. Inhaln (Children 2–12 yr): NIH Guidelines for acute asthma exacerbation via nebulization or IPPB– 0 mg/kg/dose (minimum dose 2 mg) every 20 min for 3 doses then 0–0 mg/kg (not to exceed 10 mg) every 1–4 hr as needed or 1 mg 3–4 times daily for children 10–15 kg or 2 mg 3–4 times daily for children >15 kg; Continuous nebulization– 0–3 mg/kg/hr. Inhaln Neonates: 1 mg/dose every 8 hr via nebulization or 1–2 puffs via MDI into the ventilator circuit every 6 hrs.
PURPOSE FOR TAKING THIS MEDICATION
Inhaln Prevention of exercise-induced bronchospasm. PO Used as a long-term control agent in patients with chronic/persistent bronchospasm.
PATIENT EDUCATION WHILE TAKING THIS MEDICATION
Warn patient about risk of paradoxical bronchospasm and advise patient to stop drug immediately if it occurs. Teach patient to perform oral inhalation correctly. If prescriber orders more than 1 inhalation, tell patient to wait at least 2 minutes before repeating procedure. Tell patient that use of a spacer device with appropriate inhaler may improve drug delivery to lungs. If patient is also using a corticosteroid inhaler, instruct patient to use the bronchodilator first and then to wait about 5 minutes before using the corticosteroid. Tell patient to remove canister and wash aerosol inhaler with warm, soapy water at least once a week. Warn patient not to wash or place any part of powder inhaler in water. If mouthpiece needs cleaning, advise patient to gently wipe it with dry cloth or tissue. Advise patient not to use more than prescribed and not to increase dose or frequency without consulting physician. Fatalities have been reported from excessive use. Instruct patient to report worsening symptoms.
PATIENT EDUCATION WORKSHEET
NAME OF MEDICATION, CLASSIFICATION, AND INCLUDE PROTOTYPE
MEDICATION: Azithromycin
CLASSIFICATION: o Therapeutic Class: agents for atypical mycobacterium, anti-infectives o Pharm. Class: macrolide PROTOTYPE: Erythromycin
SAFE DOSE OR DOSE RANGE, SAFE ROUTE
Patient Dose: azithromycin elixer 190 mg orally now, followed by 95 mg once daily for four days. o Recommended dosage is 10 mg/kg (not to exceed 500 mg/dose) on 1st day, then 5 mg/kg once daily (not to exceed 250 mg/dose) for 4 more day SAFE DOSAGE: 19kg10mg = 190mg for first dose / 19kg5= 95mg next 4 days
Pneumonia/Pertussis– PO (Children ≥ 6 mo): 10 mg/kg (not to exceed 500 mg/dose) on 1st day, then 5 mg/kg once daily (not to exceed 250 mg/dose) for 4 more days. Pharyngitis/tonsilitis– 12 mg/kg once daily for 5 days (not to exceed 500 mg/dose); Acute bacterial sinusitis– 10 mg/kg once daily for 3 days. Community-Acquired Pneumonia PO (Children >6 mo): 10 mg/kg on 1st day, then 5 mg/kg once daily for 4 more days. PURPOSE FOR TAKING THIS MEDICATION
Treatment of the following infections due to susceptible organisms: Upper respiratory tract infections, including streptococcal pharyngitis, acute bacterial exacerbations of chronic bronchitis and tonsillitis, Lower respiratory tract infections, including bronchitis and pneumonia, Acute otitis media, Skin and skin structure infections, Nongonococcal urethritis, cervicitis, gonorrhea, and chancroid.
PATIENT EDUCATION WHILE TAKING THIS MEDICATION
Instruct patients to take medication as directed and to finish the drug completely, even if they are feeling better. Take missed doses as soon as possible unless almost time for next dose; do not double doses. Advise patients that sharing of this medication may be dangerous. Instruct patient not to take azithromycin with food or antacids. May cause drowsiness and dizziness. Advise patient to use sunscreen and protective clothing to prevent photosensitivity reactions. Advise patient to report symptoms of chest pain, palpitations, yellowing of skin or eyes, or signs of superinfection (black, furry overgrowth on the tongue; vaginal itching or discharge; loose or foul-smelling stools) or rash. Instruct patient to notify health care professional if fever and diarrhea develop, especially if stool contains blood, pus, or mucus. Advise patient not to treat diarrhea without advice of health care professional. Advise patients being treated for nongonococcal urethritis or cervicitis that sexual partners should also be treated. Instruct parents, caregivers, or patient to notify health care professional if symptoms do not improve
PATIENT EDUCATION WORKSHEET
PATIENT EDUCATION WORKSHEET
NAME OF MEDICATION, CLASSIFICATION, AND INCLUDE PROTOTYPE
MEDICATION: Cefuroxime axetil
CLASSIFICATION: o Therapeutic class: Anti bacterial o Pharm Class: cell wall inhibitor second generation Cephalosporin
PROTOTYPE: Cefazolin SAFE DOSE OR DOSE RANGE, SAFE ROUTE Patient Dose: cefuroxime 475 mg IV piggyback over 30 minutes q8h. Recommended dosage is IV (Children and Infants >3 mo): Most infections– 50–100 mg/kg/day divided every 6–8 hr (maximum dose 6 g/day). SAFE DOSAGE: 19kg*50mg to 100mg/kg/day = 950mg to 1900mg /3 = 316 mg to 633 per dose
PO (Children 3 mo–12 yr): Otitis media, acute bacterial maxillary sinusitis, impetigo– 250 mg every 12 hr IM IV (Children and Infants >3 mo): Most infections– 50–100 mg/kg/day divided every 6–8 hr (maximum dose 6 g/day). Bone and joint infections– 150 mg/kg/day divided every 8 hr (maximum dose 6 g/day) PURPOSE FOR TAKING THIS MEDICATION
Treatment of: Respiratory tract infections, Skin and skin structure infections, Bone and joint infections (IV), Urinary tract infections, Gynecological infections, Septicemia (IV), Otitis media (PO), Meningitis (IV), Lyme disease (PO)
PATIENT EDUCATION WHILE TAKING THIS MEDICATION
Instruct patient to take medication around the clock at evenly spaced times and to finish medication completely, even if feeling better. Take missed doses as soon as possible unless almost time for next dose; do not double doses. Advise patient that sharing of this medication may be dangerous. Advise patient to report signs of superinfection (furry overgrowth on the tongue, vaginal itching or discharge, loose or foul- smelling stools) and allergy. Instruct patient to notify health care professional if fever and diarrhea develop, especially if stool contains blood, pus, or mucus. Advise patient not to treat diarrhea without consulting health care professional
Date Student Assigned vSim
Initials: SV Diagnosis
Pneumonia
Asthma
HCP: N/A Isolation: Droplet
(until cultures are
back)
IV Type: 22 guage Critical Labs
WBC: 20.
Plt: 457
Other Services
Age 5yrs Length of Stay:
As of 1/26/
Consults:
Respiratory therapy
Speech therapy
Dietary
Child team
Fall Risk: High Location at left
axillary. Bandage is
clean dry and intact ,
infucsing as
expected
M/F: F Allergies: NKA Transfer: +1 Fluid/Rate
** Potassium
Chloride in 5%
Dextrose Injectionat
61mL per hr.
Consults Needed:
Respiratory therapy
SpeechTherapy
Dietary
Code Status: N/A
* Received a 380-mL bolus of normal saline
20ml per kilo for kids (fluid bolus)
PATIENTS DOSE: 9kg*20=380mL SAFE DOSAGE
* An intravenous infusion of KLC in D5NS is infusing at 61 mL/hr
(100mL *10kg) + (50mL * 9kg) = 1000mL + 450 = 1450mL per 24hrs for maintenance fluids
PATIENTS DOSE: 61*24 = 1464mL WNL SAFE DOSAGE
Clinical Worksheet
Alerts: What are you on alert for with this patient? (Signs & Symptoms)
1. Decrease n SpO2 saturation
2. Remaining febrile despite interventions
3. Worsening B/P levels
What Assessments will focus on for this patient? (How will I identify the above signs &Symptoms?)
Continuous monitoring of SpO2 levels via monitor; admin of medication interventions as needed; keeping HOB at lest 30 degrees; encouraging coughing to clear secretions
Monitoring temperature 30 minutes after administration of Acetiminophen and again every hour after afebrile state is achieved.
Continuous monitoring via non-invasive B/P cuff; assessment of pain levels ; Assessment of anxiety levels
List Complications may occur related to dx, procedure, comorbidities:
- Aspiration
- Hypoxia; neurological damage
- Atelectasis
What nursing or medical interventions may prevent the above Alert or complications?
- Swallow study; close monitoring of food, drink and excretions
- Admin of nebulizer treatments and O2 as needed
- Monitoring and auscultations of breath sounds and O2 levels 4. Neuro checks done to establish a baseline and reassess with each shift.
Management of Care: What needs to be done for this Patient Today?
Afebrile state needs to be achieved
O2 saturation of 94% or higher maintained
Reduction and elimination of pain achieved
Swallow assessments to be done
Parent education on asthma and pneumonia to be
delivered
- Adequate fluid levels maintained
Priorities for Managing the Patient’s Care Today
- Assess dehydration status via CBC, Urinanalysis and strict I/O
- Assess patient and caregiver knowledge of pneumonia and asthma control
- Maintaining adequate SpO2 levels
- Controlling pain and anxiety levels for duration of care
What aspects of the patient care can be Delegated and who can do it? VS can be monitored and reported by the UAP I/O can be calculated by UAP Respiratory therapy can assist in stabilizing respirations
Sabrina Vasquez v Sim Complete Care Plan
Course: Nursing Care of the Childbearing Family (NURS 125)
University: Raritan Valley Community College




- Discover more from: