
- Information
- AI Chat
Cardiovascular Shadowhealth Tina Jones Documentation
Family Nurse Practitioner Ii (NUR 535)
Southern Connecticut State University
Recommended for you



Students also viewed
- Heent Shadowhealth Tina Jones Objective Data
- Shadow Health Gastrointestinal Tina Jones Objective Assessment
- Heent Shadowhealth Tina Jones Subjective
- Mental Health Shadowhealth Tina Jones Documentation
- Focused Exam-Abdominal Pain Esther Parks Shadowhealth Objective
- Gastrointestinal Tina Jones Subjective Shadowhealth
Related documents
- Focused Exam-Abdominal Pain Esther Parks Shadowhealth Subjective
- Respiratory Shadowhealth Tina Jones Documentation
- Focused Exam-Chest Pain Brian Foster Shadowhealth Subjective
- Focused Exam-Abdominal Pain Esther Parks Shadowhealth Documentation
- Respiratory Shadowhealth Tina Jones Subjective
- Shadow Health Cardiovascular Tina Jones
Preview text
1/
Cardiovascular Results | Turned In
Documentation / Electronic Health Record
Document: Provider Notes
Student Documentation Model Documentation
Your Results
Overview
Transcript
Subjective Data Collection
Objective Data Collection
Education & Empathy
Documentation
Document: Provider Notes
2/
Student Documentation Model Documentation
Subjective
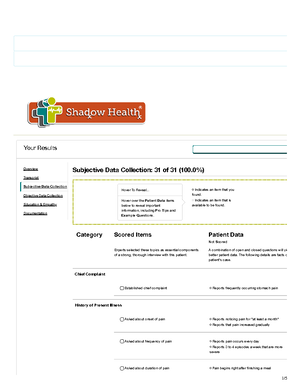
Ms. Jones is a pleasant 28-year-old African American woman w presented to the clinic with complaints of 3-4 episodes of rapid rate over the last month. She is a good historian. She describe these episodes as <thumping in her chest= with a heart rate tha <way faster than usual=. She does not associate the rapid hear with a speciûc event, but notes that they usually occur about o per week in the morning on her commute to class. The episode generally last between 5 and 10 minutes and resolve spontane She does not know her normal heart rate or her heart rate durin these episodes. She denies chest pain during the episodes, bu does endorse discomfort of 3/10 which she attributes to assoc anxiety regarding her rapid heart rate. She denies shortness of breath. She denies any association of symptoms with exertion. has no known cardiac history and has never had episodes prio this last month. She has not attempted any treatment at home states that she is only coming to the clinic today because her f has expressed concern regarding these episodes.
Social History: Ms. Jones has a job at a copy and shipping sto is a student at Shadowville Community College. She states tha has been feeling more <stressed= lately due to her school and w She has been feeling tired at the end of the day. She denies an speciûc changes in her diet recently, but notes that she has no drinking as much water as her normal. Breakfast is usually a m or pumpkin bread, lunch is a sandwich, dinner is a homemade of a meat and vegetable, snacks are French fries or pretzels. O the past month she has increased her consumption of diet sod <energy= drinks due to her feelings of tiredness. She generally d 2 energy drinks before class to <keep her focused= but states t they also make her <jittery=. She denies use of tobacco, alcoho illicit drugs. She does not exercise.
Review of Systems: General: Denies changes in weight, but complains of end of day fatigue. She denies fevers, chills, and sweats. She complains of intermittent dizziness.
Cardiac: Denies a diagnosis of hypertension, but states that s has been told her blood pressure was high in the past. She che at CVS periodically. At last check it was <140/80 or 90=. She de known history of murmurs, angina, previous palpitations, dyspn exertion, orthopnea, paroxysmal nocturnal dyspnea, or edema has never had an EKG.
Respiratory: She denies shortness of breath, wheezing, cough sputum, hemoptysis, pneumonia, bronchitis, emphysema, tuberculosis. She has a history of asthma, last hospitalization w age 16 for asthma, last chest XR was age 16.
Hematologic: She denies history of anemia, easy bruising or bleeding, petechiae, purpura, or blood transfusions.
General: Ms. Jones is a pleasant, obese 28-year-old African American woman in no acute distress. She is alert and oriented maintains eye contact throughout interview and examination.
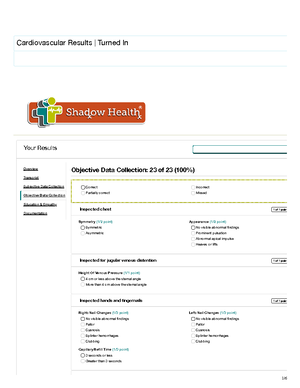
Cardiovascular: PMI is non-displaced, brisk and tapping, diam 2 cm. Regular rate and rhythm, S1 and S2 present, no murmur rubs, gallops, clinics, precordial movements. Pulses 2+ and eq bilaterally in upper extremities and lower extremities without th No temporal, carotid, abdominal aorta, femoral, iliac, or renal b No JVD. Capillary reûll < 3 seconds. No peripheral edema. EKG regular sinus rhythm, no ST changes. ABI is 0.
Respiratory: Chest is symmetrical with respirations; no physic abnormalities present on chest wall. Lung sounds clear to auscultation without wheezes, crackles, or cough.
Objective
Assessment
Palpitations related to caffeine and/or anxiety
Cardiovascular Shadowhealth Tina Jones Documentation
Course: Family Nurse Practitioner Ii (NUR 535)
University: Southern Connecticut State University


Recommended for you
Students also viewed
- Heent Shadowhealth Tina Jones Objective Data
- Shadow Health Gastrointestinal Tina Jones Objective Assessment
- Heent Shadowhealth Tina Jones Subjective
- Mental Health Shadowhealth Tina Jones Documentation
- Focused Exam-Abdominal Pain Esther Parks Shadowhealth Objective
- Gastrointestinal Tina Jones Subjective Shadowhealth
Related documents
- Focused Exam-Abdominal Pain Esther Parks Shadowhealth Subjective
- Respiratory Shadowhealth Tina Jones Documentation
- Focused Exam-Chest Pain Brian Foster Shadowhealth Subjective
- Focused Exam-Abdominal Pain Esther Parks Shadowhealth Documentation
- Respiratory Shadowhealth Tina Jones Subjective
- Shadow Health Cardiovascular Tina Jones