
- Information
- AI Chat
Mental Health Shadowhealth Tina Jones Documentation
Family Nurse Practitioner Ii (NUR 535)
Southern Connecticut State University


Students also viewed
- Focused Exam-Chest Pain Brian Foster Shadowhealth Objective
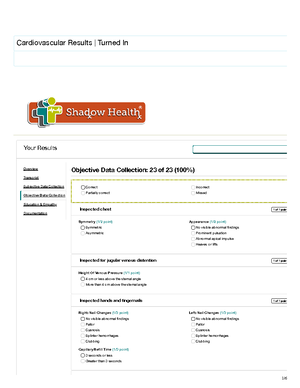
- Cardiovascular Shadowhealth Tina Jones Objective
- Focused Exam-Abdominal Pain Esther Parks Shadowhealth Objective
- Focused Exam-Cough Danny Rivera Shadowhealth Objective
- Shadow Health Gastrointestinal Tina Jones Documentation
- Tina Jones Shadowhealth Mental Health Subjective
Related documents
- Focused Exam-Cough Danny Rivera Shadowhealth Documentation
- Respiratory Shadowhealth Tina Jones Objective
- Focused Exam-Chest Pain Brian Foster Shadowhealth Documentation
- Focused Exam-Abdominal Pain Esther Parks Shadowhealth Documentation
- Heent Shadowhealth Tina Jones Documentation
- Focused Exam-Cough Danny Rivera Shadowhealth Subjective
Preview text
1/
Mental Health Results | Turned In
Documentation / Electronic Health Record
Document: Provider Notes
Student Documentation Model Documentation
Your Results
Overview
Transcript
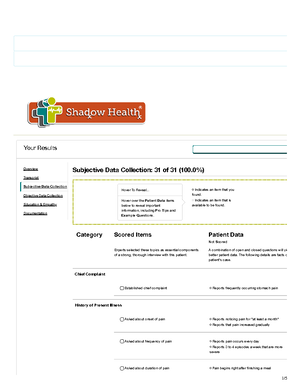
Subjective Data Collection
Objective Data Collection
Education & Empathy
Documentation
Document: Provider Notes
2/
Student Documentation Model Documentation
HPI: Ms. Jones presents to the clinic complaining of difficulty sleeping which she notes to have started 1 month ago. She sta that her sleep is <shallow and not restful=. She complains of diffi falling asleep at least 4 or 5 nights per week, but states that sh able to stay asleep without difficulty. On average she sleeps 4 o hours per night and awakens at 8:00am daily. She states that s has a fairly consistent schedule on weekdays and weekends. S does not take any prescription or over the counter sleep aids. S limits screen time prior to bed and does not ingest caffeine afte 4pm daily. She endorses decreased feelings of sleepiness over past month. She denies difficulties awaking, but does not feel r in the morning and has daytime fatigue (rates 5/10 severity), restlessness, and irritability (rates 2/10 severity). She does not naps.
Social History: She states that she has some stress related to h upcoming examinations and her impending job search upon graduation. She states that she has a strong support system m up of friends and family and she is active in her church. She sta that she copes with stress by staying organized. She enjoys rea and watching television (1-2 hours per day). She states that he father died in a car accident a year and a half ago, which was difficult for her and she experienced some difficulties with sleep that time as well. She denies use of tobacco. She drinks approximately 10-12 alcoholic beverages per month, but never than 3 per sitting and does not note any impact on her sleep. S has used marijuana in the past, but no current use and denies illicit drugs. She does not exercise regularly, but states that her somewhat active and she walks 5-15 minutes daily. She drinks diet colas per day.
Family History: Denies any history of known sleep disorders or psychiatric disorders.
Review of Systems:
- General: Denies changes in weight, weakness, fever, chills, an night sweats. Does complain of increasing daytime fatigue.
- Neurologic: Denies loss of sensation, numbness, tingling, trem weakness, paralysis, fainting, blackouts, or seizures. Endorses changes in concentration and sleep. Denies changes or difficul coordination.
- Psychiatric: States that her mood has been <off= and she doe feel like herself. She does complain of increased anxiety related upcoming exams and job search. She has no history of depres but does state that she feels helpless and notes that her performance at work and school is beginning to decline. She d tension or memory loss. No past suicide attempts. Denies suic homicidal ideation.
Subjective
Objective
Assessment Sleep disturbance related to anxiety
Mental Health Shadowhealth Tina Jones Documentation
Course: Family Nurse Practitioner Ii (NUR 535)
University: Southern Connecticut State University



Recommended for you
Students also viewed
- Focused Exam-Chest Pain Brian Foster Shadowhealth Objective
- Cardiovascular Shadowhealth Tina Jones Objective
- Focused Exam-Abdominal Pain Esther Parks Shadowhealth Objective
- Focused Exam-Cough Danny Rivera Shadowhealth Objective
- Shadow Health Gastrointestinal Tina Jones Documentation
- Tina Jones Shadowhealth Mental Health Subjective
Related documents
- Focused Exam-Cough Danny Rivera Shadowhealth Documentation
- Respiratory Shadowhealth Tina Jones Objective
- Focused Exam-Chest Pain Brian Foster Shadowhealth Documentation
- Focused Exam-Abdominal Pain Esther Parks Shadowhealth Documentation
- Heent Shadowhealth Tina Jones Documentation
- Focused Exam-Cough Danny Rivera Shadowhealth Subjective